


 Sign Out
Sign Out

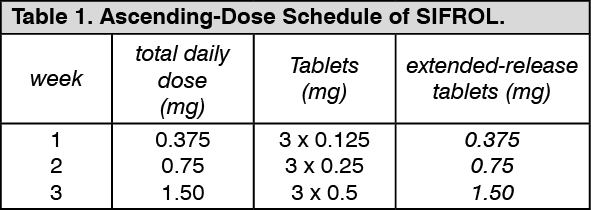
Parkinson's disease: Dosage: Initial Treatment: As shown in Table 1 as follows, dosages should be increased gradually from a starting dose of 0.375 mg per day and then increased every 5-7 days. Providing patients do not experience intolerable side effects, the dosage should be titrated to achieve a maximal therapeutic effect. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIf a further dose increase is necessary, the daily dose should be increased by 0.75 mg at weekly intervals up to a maximum dose of 4.5 mg per day.
Patients already taking SIFROL tablets may be switched to Sifrol extended-release tablets overnight, at the same daily dose.
Maintenance treatment: The individual dose should be in the range of 0.375 mg to a maximum of 4.5 mg per day. During dose escalation in pivotal studies both in early and advanced disease efficacy was observed starting at a daily dose of 1.5 mg. This does not preclude that in individual patients doses higher than 1.5 mg per day can result in additional therapeutic benefit.
This applies particularly to patients with advanced disease where a reduction of the levodopa therapy is intended.
Treatment discontinuation: SIFROL tablets and extended-release tablets should be tapered off at a rate of 0.75 mg per day until the daily dose has been reduced to 0.75 mg. Thereafter the dose should be reduced by 0.375 mg per day (see Precautions).
Missed dose: When the intake of a dose is missed, SIFROL extended-release tablets should be taken up to 12 hours after the regularly scheduled time. After 12 hours, the missed dose should be left out and the next dose should be taken on the following day at the next regularly scheduled time.
Dosing in patients with concomitant levodopa therapy: In patients with concomitant levodopa therapy it is recommended that the dosage of levodopa is reduced during both dose escalation and maintenance treatment with SIFROL. This may be necessary in order to avoid excessive dopaminergic stimulation.
Dosing in patients with renal impairment: The elimination of pramipexole is dependent on renal function. The following dosage schedule is suggested for initiation of therapy: Patients with a creatinine clearance above 50 ml/min require no reduction in daily dose or dosing frequency.
Tablets: In patients with a creatinine clearance between 20 and 50 ml/min, the initial daily dose of SIFROL tablets should be administered in two divided doses, starting at 0.125 mg twice a day (0.25 mg daily). A maximum daily dose of 2.25 mg pramipexole should not be exceeded.
In patients with a creatinine clearance less than 20 ml/min, the daily dose of SIFROL tablets should be administered in a single dose, starting at 0.125 mg daily. A maximum daily dose of 1.5 mg pramipexole should not be exceeded.
If renal function declines during maintenance therapy reduce SIFROL daily dose by same percentage as decline in creatinine clearance, i.e. if creatinine clearance declines by 30%, then reduce SIFROL daily dose by 30%. The daily dose can be administered in two divided doses if creatinine clearance is between 20 and 50 ml/min and as a single daily dose if creatinine clearance is less than 20 ml/min.
Extended-release tablets: In patients with a creatinine clearance between 30 and 50 ml/min, treatment should be started with 0.375 mg SIFROL extended-release tablets every other day. Caution should be exercised and careful assessment of therapeutic response and tolerability should be made before increasing to daily dosing after one week. If a further dose increase is necessary, daily doses should be increased by 0.375 mg pramipexole at weekly intervals up to a maximum dose of 2.25 mg pramipexole per day.
No data are available for the treatment of patients with a creatinine clearance below 30 ml/min with SIFROL extended-release tablets. The use of SIFROL tablets should be considered.
If renal function declines during maintenance therapy, the recommendations given previously should be followed.
Dosing in patients with hepatic impairment: Dose reduction is not considered necessary in patients with hepatic impairment.
Method of Administration: Tablets: The tablets should be taken orally, swallowed with water, and can be taken either with or without food.
The daily dosage is administered in equally divided doses 3x per day.
Extended-release tablets: The extended-release tablets should be taken once daily at about the same time each day. The extended-release tablets should be swallowed whole with water, and must not be chewed, divided or crushed. The extended-release tablets may be taken with or without food.
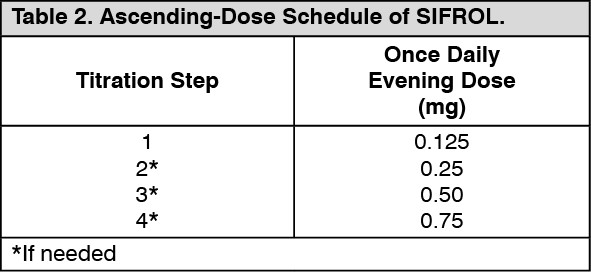
Restless Legs Syndrome: Dosage: The recommended starting dose of SIFROL is 0.125 mg taken once daily 2-3 hours before bedtime. For patients requiring additional symptomatic relief, the dose may be increased every 4-7 days to a maximum of 0.75 mg per day (as shown in Table 2 as follows). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment discontinuation: SIFROL can be discontinued without tapered dose reduction. In a 26-week placebo controlled clinical trial, rebound of RLS symptoms (worsening of symptom severity as compared to baseline) was observed in 10% of patients (14 out of 135) after abrupt discontinuation of pramipexole. This effect was found to be similar across all doses.
Dosing in patients with renal impairment: The elimination of SIFROL is dependent on renal function and closely related to the creatinine clearance. Based on a pharmacokinetic study in renally impaired subjects, patients with a creatinine clearance above 20 ml/min require no reduction in daily dose. The use of SIFROL in RLS patients with renal impairment has not been studied.
Dosing in patients with hepatic impairment: Dose reduction is not considered necessary in patients with hepatic impairment, as approx. 90% of absorbed drug is excreted through the kidneys.
Dosing in children and adolescents: Safety and efficacy of SIFROL have not been established in children and adolescents up to 18 years.
Method of Administration: The tablets should be taken orally, swallowed with water, and can be taken either with or without food.